Trusted Dentist-Owned Care for Growing Smiles
Commerce Park Children’s Dentistry and Orthodontics is proudly dentist owned, meaning every decision is made with your child’s health and comfort in mind. With a team dedicated to personalized, compassionate care, families can trust they’re receiving genuine expertise and a warm, welcoming experience every visit.

Meet Your Dentists
At Commerce Park Children’s Dentistry and Orthodontics, our dedicated team is committed to delivering exceptional care with compassion and respect. Get to know our pediatric dentists: Dr. Andrew Spadinger, Dr. Mary Ritter, who is a dual specialist in both pediatric dentistry and orthodontics, Dr. Jessica Corriel, Dr. Meenakshi Madhu and Dr. Stephanie Fanelli. Our team is focused on promoting lifelong healthy dental habits in a friendly and soothing atmosphere. Begin your journey with us today and experience the difference our exceptional care can make!
Meet Your Dentists
At Commerce Park Children’s Dentistry and Orthodontics, our dedicated team is committed to delivering exceptional care with compassion and respect. Get to know our pediatric dentists: Dr. Andrew Spadinger, Dr. Mary Ritter, who is a dual specialist in both pediatric dentistry and orthodontics, Dr. Jessica Corriel and Dr. Meenakshi Madhu. Our team is focused on promoting lifelong healthy dental habits in a friendly and soothing atmosphere. Begin your journey with us today and experience the difference our exceptional care can make!





Insurance Participation & Coverage Assistance
At Commerce Park Children’s Dentistry and Orthodontics, we believe every child deserves quality dental care. We participate with Delta PPO, Anthem Blue Cross, Cigna, Husky and UnitedHealthcare PPO! Dental plan details can vary, so we encourage you to contact our administrative team to confirm your specific coverage and benefits. We’re happy to help you navigate your plan and maximize your benefits!

Pediatric Services
Creating Healthy Smiles for Your Child’s Future
We are proud to provide comprehensive pediatric dental services so that your child receives the best care from infancy through adolescence. Our skilled pediatric dentists offer personalized care tailored to each child’s unique needs, focusing on preventative care, early detection and gentle treatments. We strive to make every visit stress-free and enjoyable, helping your child develop a positive attitude toward dental health while achieving a healthy, beautiful smile.


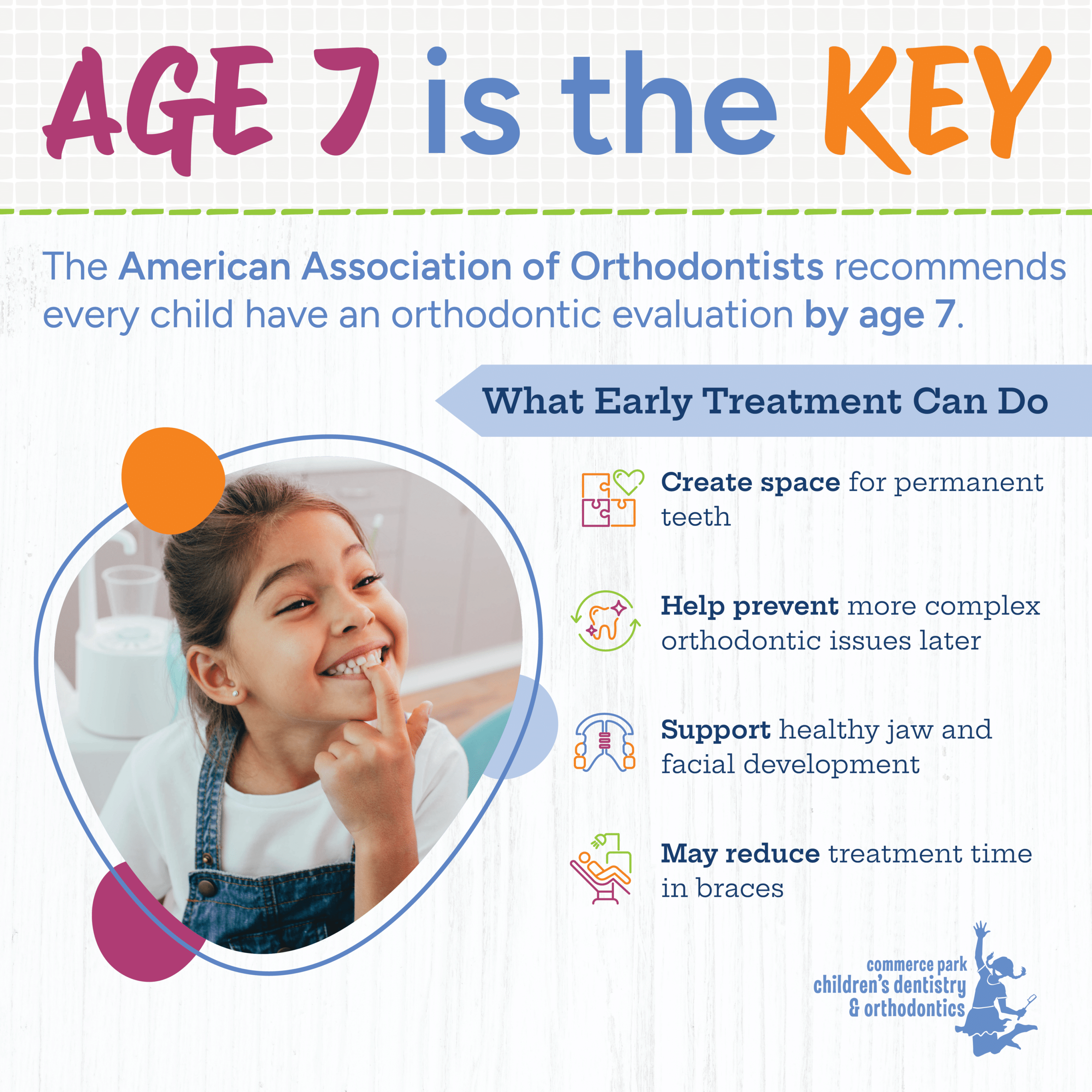
Orthodontic Care For All Ages
Advanced Orthodontic Techniques for Lasting Results
Our practice provides a wide range of modern orthodontic treatments designed to correct dental issues and improve aesthetics. From early orthodontic treatment to adolescent orthodontic treatment, traditional braces to clear aligners, we utilize the latest technology to achieve the best possible outcomes. With a focus on comfort and convenience, we ensure that your orthodontic journey is smooth and effective while helping you achieve the smile you’ve always wanted at any age.













Read Our Blog
Stay Up To Date
Explore our blog to stay informed about the latest tips, news, and insights on pediatric dentistry and orthodontics. From expert advice on maintaining your child’s oral health to updates on new treatments and technologies, our blog is your go-to resource for keeping your family’s smiles healthy and bright.